Abstract
The numbers of persons with disabilities (PWDs) worldwide, and particularly in the developing countries, are increasing due to wars, conflicts, vehicular accidents, chronic diseases, mental impairment, birth defects and malnutrition. Many of these PWDs face participation-restriction in activities of life. Thus, rehabilitation seeks to remove or reduce the handicapping effects of disability and lead to an improvement in the quality of life of the PWDs. Therefore, This paper reviews the institutional-based rehabilitation (IBR) and community-based rehabilitation (CBR) approaches for rehabilitation. Other areas entail in the paper are conceptual definitions of rehabilitation and persons with disabilities. The paper ends with a conclusion as well.
Keywords: Persons with Disabilities (PWDs), Institutional-Based Rehabilitation (IBR), Community-Based Rehabilitation (CBR).
Introduction
There are different responses to the issues associated with disabilities. Clearly, eliminating discrimination, segregation and negative attitudes are necessary responses. But in developing countries particularly, the notions of prevention and rehabilitation are seen as vitally important because so many impairments can be avoided. Many have dichotomized between prevention and rehabilitation as two mutually exclusive techniques, with rehabilitation being a second-rate alternative. Certainly, prevention is the most desirable attack against many disabling conditions, such as polio, which can be combated by vaccination; or cerebral palsy, which is often caused by poor pre- and post-natal care. Disability specialists have asserted that up to 50% of some types of disabilities could be prevented by immunizations, environmental improvements and better overall health care (Lambo and Sartorius, 2013). Many diseases and conditions that result in disabilities cannot be easily prevented and many cannot be prevented at all, no matter how developed a country is or how comprehensive its preventative health-care system.
The focus of rehabilitation on the individual rather than on the wider community and the physical environment has major implications. Because it helps to keep the problems hidden from the public eye, so that policy makers, planners, politicians and others are less likely to take the needs of persons with disabilities into account. Because the problem is seen to lie within the individual and in her/his limitations, the solution must also logically be sought at this level, that is, in individual adjustment, rather than in environmental accommodation or modification. Therefore, the institution-based rehabilitation (IBR) approach of persons with disabilities has emphasized segregated institutional care, and has largely neglected the need both to integrate persons with disabilities into their wider community, and for community attitudes themselves to be rehabilitated or changed to facilitate this integration. Alternatively, the community-based rehabilitation (CBR) approach is conceived as a strategy within community development for the rehabilitation, equalization of opportunities, and social integration of all persons with disabilities. CBR is implemented through the combined efforts of persons with disabilities themselves, their families and communities, and the appropriate health, education, vocational and social services (Tompett, 2009).
Persons with Disabilities (PWDs)
Disability is an umbrella term for impairments, activity limitations, and participation restrictions, denoting the negative aspects of the interaction between an individual (with a health condition) and that individual’s contextual factors (environmental and personal factors) (WHO, 2011). Persons with disabilities (PWDs) therefore include those who have long-term physical, mental, psycho-social, intellectual or sensory impairments resulting from any physical or mental health conditions which in interaction with various barriers, may hinder their full and effective participation in society on an equal basis with others (UN, 2008).
People with disabilities throughout the world experience discrimination and segregation. Although in more developed countries the disability community has been championing accessibility and appropriate community supports, people with disabilities in less developed countries often have little access to any services or supports at all (Mia, 1983).
The overall prevalence of persons with disabilities across the world has been estimated at nearly 500 million persons, approximately 75% of them residing in the developing world (Lundgren & Nordholm, 2018). The exact number of persons with disabilities in the developing world is hard to ascertain, due both to difficulties in estimation and to the notion that disability itself is a social construct that is difficult to define. Nevertheless, the rate of disability has both placed great financial strains on the health-care systems of developing countries and has created a large class of non-working populations.
Poor overall health conditions, poverty and malnutrition, chronic diseases, wars and conflicts as well as accidents are major factors in causing the higher rates of disability in less developed countries. The most common causes of childhood disability in these countries are malnutrition of pregnant mother and child (resulting in iodine deficiency), injuries before and during birth, exposure to toxic substances and infectious diseases (Hammerman, 2015). These factors, many of which can be avoided, result in a large number of children being afflicted with paralysis, stunted growth, deafness, blindness, epilepsy and learning disabilities among others (Lambo & Sartorius, 2013).
Concept of Rehabilitation
Rehabilitation is not only concerned with physical or functional restoration/compensation of persons with disabilities by injury or disease. Attention is also given to the total quality of life in terms of wellness, happiness and satisfaction in fulfilling the demands, needs, and capacities of human existence in orientation, freedom of movement, independence, expression of self (with respect to age, sex and culture), relationship and ability to ensure independent economic existence. After a serious injury, illness or surgery, one needs to recover slowly. There is the need to regain strength, to relearn skills or find new ways of doing things one did before. This is the process of rehabilitation (Mock, 2003).
Children who are born with disabilities need stimulation for development and adaptation – habilitation (Winnick, 2007), and those who acquire disabilities also need rehabilitation. Technically, therefore, rehabilitation is a creative procedure that includes the cooperative efforts of various medical specialists, and associates in other health, technical and environmental fields, to improve the physical, mental, social and vocational aptitudes of the PWDs, with the objectives of preserving and improving their ability to live happily and productively on the same level, and with the same opportunities as their neighbors (Olaogun, 2010). In other words, it is a process of decreasing the dependence of the person with disability, by developing to the greatest extent possible, the abilities needed for adequate functioning in his individual situation in the community (Goffman, 2004).
Rehabilitation is defined by WHO as ‘all measures aimed at reducing the impact of disability and handicapping conditions, and at enabling the disabled and the handicapped to achieve social integration’ (Lundgren & Nordholm, 2018). Rehabilitation is thus suited for two circumstances: first, for situations when some sort of physical or mental impairment exists, but is amenable to treatment to improve or prevent a further condition; second, if a person has a condition that cannot be improved, but could become more independent through special assistance that builds on their abilities.
Rehabilitation of persons with disabilities may be summarized as meaning to integrate or re-integrate physically, sensorially, mentally and/or psychologically persons with disabilities into as full and as normal life roles as is possible. Rehabilitation in its fullest sense necessitates, on the one hand, maximizing the physical and mental fitness of individuals and their capacity to work and to enjoy life, through interventions ranging from the medical and paramedical to counseling and vocational training and job placement; and, on the other hand, promoting the accessibility and openness of the physical and social environment to persons with disabilities (Oliver, 2001).
Institutional-Based Rehabilitation (IBR)
Institutional-based rehabilitation services are segregated institutional care, which include medical and vocational rehabilitation centers, residential homes, special schools with therapy and nursing care, sheltered workshops and day centers, to name the most salient, have formed the backbone of rehabilitation services in developed countries, supported to differing degrees by financial and material benefits, counseling and other support services in the community. However, for PWDs living at home, and for their families and friends living or working with them, access to support services may vary enormously. Many people, particularly those severely mentally handicapped, remain in long term residential care despite mounting evidence of the inadequacies of many such institutions (Bose, 2003).
While this conception of rehabilitation can be appropriate in many circumstances, many less developed countries, following the lead of more developed countries, have adopted an institutional model of rehabilitation (Marincek, 2008). The institutional model relies on professionally trained specialists who use state-of-the art equipment to provide intensive rehabilitation to people with disabilities. Treatment is provided in institutions, usually located in major urban areas (Malafatopoulos, 2006). As health and rehabilitation are viewed in the institution-based model as a medical problem rather than also as a social problem, rehabilitation is treated as simply a medical service (WHO, 1986).
However, an institution-based rehabilitation program may not be suitable for many developing countries for several reasons. First, these institutions are enormously expensive, requiring large capital outlays for sophisticated equipment, facilities and professional staff. Most people with disabilities, who are often the poorest of the poor, are not able to afford this expensive institutional care, and thus have no access to its services (Malafatopoulos, 2006). Second, these institutions are almost always located in the cities, away from the rural population (Mia, 2016). Third, the high-tech equipment used in these rehabilitation institutions is expensive, and requires highly trained specialists to run it (Finkenflugel, 2011). Thus, developing countries must trade a large amount of scarce resources for equipment, personnel, spare parts and training in order to serve only a small proportion of their population (Mia, 2016). Furthermore, the Western concern about the segregation caused by institution-based services is also a valid concern in less developed countries. The institutional method of providing services to people with disabilities is contraindicated for many situations.
In this category, general or specialized services are offered in an institution or home for the PWDs. General institutions include centers that provide services for people with all types of disability. Specialized ones include homes for children with physical disability, e.g., Atanda Olu School, Surulere, Lagos and Cheshire Home Oluyole, Ibadan, all in Nigeria. Rehabilitation Centre, Moniya, Ibadan, is also an institution-based rehabilitation center, with active rehabilitation services and vocational training for spinal cord injury victims. The institute also provides out-patient and in-patient services, and long-term boarding. An example of this is Modupe Cole Home for the Handicap, Akoka, Lagos. There are regular physiotherapy services for the cerebral palsy children in this home (Dube, 2005).
Community-Based Rehabilitation (CBR)
The World Health Organization (WHO) has proposed the Community-based Rehabilitation model (CBR) as an appropriate model for developing countries to provide basic rehabilitation services to its citizens. The CBR model, derived from WHO’s Primary Health Care model (PHC), promotes the use of community resources and personnel to provide basic rehabilitation services in a low-cost, yet highly accessible manner. CBR is currently being adopted rapidly by both less and more developed countries (Lightfoot, 2016).
An alternative approach to Institutional Based Rehabilitation (IBR) is Community Based Rehabilitation (CBR) which has the notion that:
If rehabilitation is to reach all those in need in the developing countries, there must be a large-scale transfer of knowledge about disabilities and skills in the rehabilitation of people with disabilities to their families and members of the community.
For rehabilitation to be successful, communities must recognize and accept that people with disabilities have the same rights as other human beings. Rehabilitation therefore needs to aim at bringing about this required attitude- change in communities. It has been found that this change in attitude is most effectively brought about when communities themselves take on the task of rehabilitating their members who have disabilities. CBR is a strategy that seeks to ensure that people with disabilities are involved in the development of their community by having equal access to rehabilitation and other services and opportunities – health, education and income; as do other members of the society (Lightfoot, 2016).
The targets of the CBR programme are: people with disabilities, families of people with disabilities, organizations of people with disabilities, local, regional (state) and national (federal) governments, international organizations, non-governmental organizations, professionals in health sciences and other fields and the private sector (business and industry). Likewise, the system components of the CBR include: technology, service delivery and community involvement and close cooperation with organizations of people with disabilities and parents of children with disabilities (Marincek, 2008).
The rehabilitation places the primary focus on community care or family care, with institutions playing a support role rather than being the main rehabilitation resource. Community based rehabilitation has been promoted for several years by the WHO, UNICEF, the ILO and other international organizations, and it is gaining increasing acceptance by governments and NGOs in many developing countries. The WHO (1986) suggests that specialist rehabilitation institutions should be used for complex medical and paramedical services for acute and special needs; for research; training; workshops for more complicated aids and appliances; coordination and planning; and bases for mobile units such as eye units, amongst other possible functions. They should be the last possible stage in a referral chain starting with families and village health workers. (or equivalent), and the first stage for referral after acute, and severe injury. The aim of Rehabilitation institutions should be short term intensive care rather than long term, except in some extreme cases, and their specialist services should genuinely be available to those most in need of them.
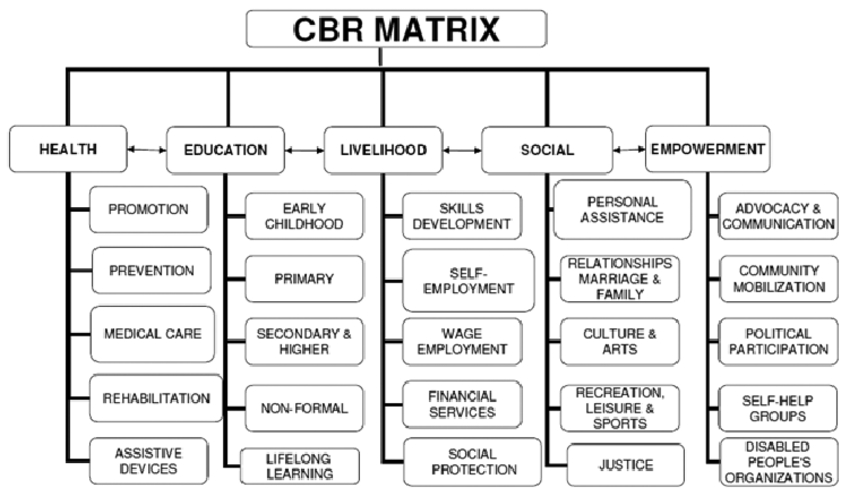
Source: WHO (1986)
The WHO concentrates mainly on the medical and paramedical aspects of rehabilitation, but a move away from institutional segregation is both possible and desirable for education and vocational rehabilitation as well. Children with disabilities can attend normal schools in the community, if they can get access to them - this means both transport to reach the school and accessible buildings. For those with special learning needs, the sensorially or mentally impaired, especially classes may be needed in some subjects, but integration in others may be feasible. Teachers in ordinary schools can be given extra training in block or day release to cope with the needs of children with disabilities; specially trained teachers can visit normal schools; simple aids can be developed to overcome a variety of problems. A problem-solving strategy can be adopted, with the central focus of maximizing the integration of children with different disabilities into as normal an educational environment as possible, and with the aim of maximizing their abilities and opportunity for normal development (Freire, 2008).
Community based rehabilitation can potentially encompass the whole range of rehabilitation services with greater success than the expensive, segregationist strategy of institutional care. The main advantages of such an approach may be summarized as follows:
it is much cheaper than institutional care, and therefore has the potential to reach all PWDs, not just a select few;
it avoids dislocating people from their communities, and the risks of institutionalization, psychological scarring, and the creation of dependence;
it trains people to cope directly with the environment in which they will live, using resources that are largely available locally;
it improves detection and referral, greatly reduces problems of transport and access, allows easy supervision and follow up, and continued support for the whole family;
it can ensure that PWDs learn useful skills that are directly applicable in their environment, thus promoting their self-sufficiency and also their capacity to contribute directly to their own society;
it promotes community and rural development by creating jobs: rehabilitation workers can be drawn from the local community, many simple aids and appliances can be produced locally using local materials and skills as far as possible, and PWDs themselves may be trained to work for the rehabilitation of others;
by a keeping PWDs in the community it enhances family and community understanding and acceptance of PWDs, and an understanding of the causes and treatment of impairments. This will lead to better prevention of impairments, earlier detection and treatment of potentially disabling conditions, and lessened ostracism and social handicapping of impaired individuals;
it leaves rehabilitation institutions free to concentrate on acute and severe disability or special needs requiring highly technical intervention, and on research, development, training and other functions that make rational use of specialized and scarce resources (Abdi, 2003).
Thus a well developed community based rehabilitation strategy can be seen to have major benefits for people with disabilities, for their families and for the community itself. For governments with a commitment
to the welfare and development of their people this approach provides the possibility of effective rehabilitation for all without the crippling expenditure of institutional care (Tinney, 2007).
Conclusion
It would seem that some form of community based or community orientated
rehabilitation is the only feasible strategy to attempt to meet both the immediate physical needs of persons with disabilities, and the long term goal of community conscientisation about health care, prevention of impairments, rehabilitation of the PWDs and their full acceptance into the community. Centralized institutional care fails to educate the community, and imposes further psychological stress and isolation on already stressed people, whilst rehabilitating them to cope with an environment different from their own. In the wider context, community based rehabilitation can be seen as part of the general aim of rural development, whereby resources of cash, materials, services, jobs, and, crucially, human potential are promoted in the rural areas. For people with disabilities it offers the possibility of real integration, and not the segregated rehabilitation of the institution. Different countries need a strategy appropriate to their particular constraints and demands, and one that can be developed with flexibility to meet their particular needs in ways that are culturally acceptable and practically and economically feasible.
It is to be hoped that more developing countries will experiment with and expand community rehabilitation services, and incorporate this type of strategy as the cornerstone of national policies on rehabilitation. The potential benefits extend far beyond the immediate needs of PWDs, into the enrichment and development of the general community itself, and can be identified as incorporating both humanitarian and economic considerations.
References
Abdi, O. A. (2003). Disability in Somaliland. Disability and Society 18(7), pp.911- 920.
Bose, A. (2003). "The Community Health Worker Scheme: An Indian Experiment" in Practising Health for All, Morley et al. (eds). London: Oxford Press.
Dube, P. N. (2005). Perceived Barriers to Employment Among Trained Physically Disabled People. BSW Dissertation, School of Social Work, Harare.
Finkenflugel, H. (2011). ‘Help for the Disabled – in Hospital and at Home’, World Health Forum 12: 325–30.
Freire, P. (2008). Pedagogy of the Oppressed. New York: Penguin Books, Middlesex.
Goffman, E. (2004). National Disability Policy Document. Retrieved from http://www.disability.dk/site/viewdoc.php?doc_id=208&se ction_id=6. On 18/12/2021
Hammerman, S. (2015). ‘Disabled People in the Third World: The Silent Emergency’, in D. Warms (ed.) Into the 21st Century: Selected Papers from the UCP Inter-national Conference on The Changing Rehabilitation World, pp. 103–8. New York: United Cerebral Palsy of New York City.
Lambo, T. & Sartorius, N. (2013). ‘Mental Health Programs: An International Perspective’, in T. Lambo and S. Day (eds) Issues in Contemporary International Health. New York: Plenum Medical Book Company.
Lightfoot, E. (2016). Community-based rehabilitation: A rapidly growing method for supporting people with disabilities. International Social Work, 47(4):455–468.
Lundgren, B. & Nordholm, L. (2018). ‘Community-based Rehabilitation – A Survey of Disabled in a Village in Botswana’, Disability and Rehabilitation 15(2):83–9.
Malafatopoulos, S. (2006). ‘Rehabilitation in the Third World’, in D. Warms (ed.) Into the 21st Century: Selected Papers from the UCP International Conference on The Changing Rehabilitation World, pp. 100–2. New York: United Cerebral Palsy Foundation.
Marincek, R. (2008). ‘Community-based Rehabilitation – the Challenge and Opportunity. International Disability Studies 10: 87–8.
Mia, A. (2016). ‘Community Participation: The Needed Approach to Primary and Secondary Prevention of Disability and Rehabilitation of the Disabled in Rural Communities’. International Social Work 26: 26–34.
Mock, C. S. (2003). Long-term injury related disability in Ghana. Disability and Rehabilitation, 25 (13), pp.732-741. New York City.
Olaogun, M. Z. (2010). The Oyo State Community Physiotherapy Scheme: Preventive and promotive measure in Nigeria. Physiotherapy Practice 2, pp.174-176
Oliver, M. (2001). Social Work with Disabled People. London: BASW, Macmillan.
Tinney, W. J. (2007). Medical rehabilitation in Ghana. Disability & Rehabilitation 29(11), pp.921-927.
Tompett, J. (2009). CBR in Nassarawa State: Presentation at the 47th Annual Conference of the Nigeria Society of Physiotherapy. Mallam Amino Kano Teaching Hospital, Kano.
UN (2008). United Nations Convention on the Rights of Persons with Disabilities. Geneva: UN Press.
WHO (1986). "Rehabilitation For All", in World Health Magazine, May 1984, WHO, Geneva: WHO Press.
WHO (2011). World Report on Disability, Chapter 4: Rehabilitation, 2011, p. 96–133.
Winneick, D. (2007). Disabled Village Children: A Guide to Community Health Workers, Rehabilitation Workers, and Families. Palo Alto, CA: Hesperian Foundation.
No comments:
Post a Comment